
Should Children Wear Orthotics…
That is the question most parents are asking! How do I know if or when I should introduce orthotics? So if your like me as a parent, when I’m not sure I go to google and see what info is there…. Fun times with this topic! The information on google from Allied Health Practitioners is so conflicting and therefore confusing.
Below I’ll give you some guidelines and also be honest about what we do know about foot and lower limb development.
1) Children don’t introduce a heel strike to their walking style until approx. 2.5 to 3 years of age. So before this time its difficult to see if their foot position is effecting their movement. It is during these first years of load they uptake a lot of sensory information through barefoot loading. I recommend lots of different surfaces in bare feet and shoes only for protection when surfaces can put the feet at risk of harm. eg, Hot surfaces.
Orthotics are generally not recommended before this age unless there is developmental delays. For example if your child is over 18 months and yet to start walking this is delayed. If this is the case for your child, see a Podiatrist. Don’t just fit your child into an off the shelf orthotic. Sometimes an ankle foot orthotic is a better option in these cases, so assessment is crucial.
2) Once they are 2.5 to 3 years you can start to gauge whether they are able to keep up with their peers. Are they complaining of tired feet and/or sore legs? Are they refusing to walk and wanting to be carried more? This can be a younger child’s way of describing pain or discomfort during load. Parents may intervene with an orthotic here and see whether this helps settle those behavioral changes.
3) Is your child currently experiencing diagnosed pain:
The back of their heel. ( Achilles tendon or Severs pain)
The arch ( Plantar Fascial pain)
The outside of their ankle ( Sinus tarsi pain)
The shin bone ( Shin splints)
The knee ( Patellofemoral syndrome or Osgood Schlatters)
Orthotics are recommended alongside stretch and strengthening programs to reduce pain.
Contact me for more info, happy to help.
4) Is your child hypermobile? Hypermobility is when the ligaments connecting the bones/joints are quite lax. This will mean the child can go to the end range of motion in many joints of the body including the ankle, foot and hip quite easily. Orthotic’s can help reduce the ability of those joints reaching end range of motion and thereby reduce risk of predisposing pain/syndromes associated. Just because a child has hypermobility doesn’t mean they will have pain. Parents can chose to support foot position with an orthotic.
5) Does your child have poor flexibility and/or stooped posture? Often kids with hypertonia have very tight hamstring muscles. This effects hip position by moving the pelvis forward, internally rotates the leg inside the hip socket and also effects foot position and load by pronating (rolling in) the foot further than normal gait pronation. If you head to my instagram I have a video on on to check hamstring flexibility and also a handy stretch you can do to assist your child. Orthotic’s are recommended alongside a stretching and strengthening program.
6) A lot of parents are choosing to use orthotics as a preventative tool to reduce risk of predisposing pain conditions. They look at their child’s feet and lower limb position and see the reflection of themselves or the other biological partner. Parents may have had pain themselves as child or adult. They can identify the genetic mapping passed down.
My son William is a super imposed copy of me. He has my flat feet and hypermobile knees that aided my patellofemoral syndrome. My husband and I choose to use kidzoles to support his developmental position and guide his walking and running style. Madison, our daughter is my husbands replica. We did the gender swap on genetic mapping! Again, we choose to use kidzoles as a guide for her foot development and walking style in her shoes.
How the Arch Develops
1) At 2.5- 4 years old the foot is undergoing a massive developmental process where a lot of the foots boney mass is still changing from cartilage to solid bone. Feet will appear flatter because of this.
2) At 5 years of age the navicular bone ossifies and we start to develop some arch shape.
3) At 7-8 years of age the sustinaculaum talar which is a very important lever system in our heel bone will have formed it solid shape. This funny named piece of the heel bone aids in the function of muscle working between the leg and foot. Arch profile becomes more evident.
4) Its is consider that by the age of 10 we have a formative idea of the child’s long term arch shape. Although the end development of arch shape is not 100% certain and there is considerations that this may continue to change up into adulthood.
Prevention or Pain?
So do we wait until 10 when arch shape is mostly formed or do we guide the foot development up to that age in order to improve position? You will find their are two opinions held between practitioners! Some saying to only intervene when pain occurs and others say if you can see the signs that predisposes the child to developing pain you should prevent it. That decision ultimately lies with you, the parent.
I believe there is a place for prevention with orthotics. I prefer to treat those predisposing factors rather than place the child at risk to pain pathologies. As a child presents with pain they often have a mirage of other “non-pain” symptoms like poor flexibility. Flat foot position with hypermobility. I would consider tripping, tired legs and an inability to keep up with their peers in the playground as all “non pain” symptoms that warrant involvement.
I have been working for 19 years as a Podiatrist with special interests in Sports and Peadiatrics. I’ve seen so many children present with pain, that also have the non pain symptoms or markers. Had I seen them and guided their development earlier I would have reduced the risk of developing pain in the first place. Orthotics form part of this developmental guide alongside stretching and strengthening of the lower limb muscles. Hit my insta to see a few easy exercises you can do with your kids.
When I developed the kidzoles range I wanted to provide an orthotic for each age group that guided the foot and lower limb mechanics. Little pivot points within the orthotics that allowed the extrinsic leg to foot muscles to engage at the correct moment for movement. A child at age 3 does not have the same foot development as a child of 8 years of age, and therefore will take load differently. I also considered the more common pain pathologies per age group and made sure these orthotics were pitched at the correct points of foot mechanics to reduce risk.

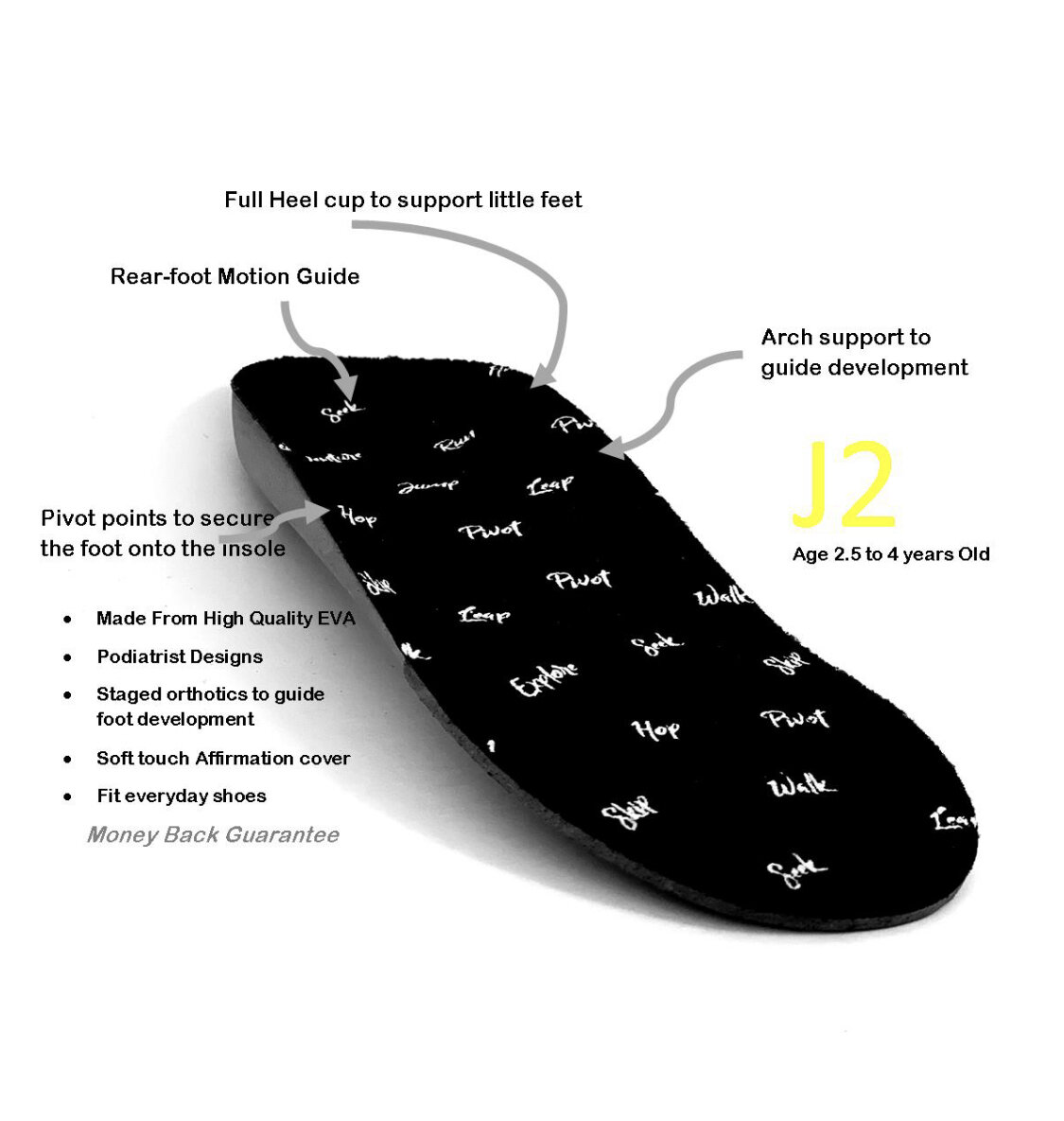




I’m really proud of these designs. Kidzoles are functional orthotic devices. They have triggers for the foot to act around better pivot points and pitch. I was very aware to support the muscle function between the leg and foot, while not over correcting the plantar arches. We still want those intrinsic muscles to work and become strong. I truly believe that different orthotic designs should be considered for different age groups so we encourage the development and strength of the lower limb in those kids that just need a little help. We need our children outdoors, playing sports, being active and developing muscle endurance and memory. Kidzoles are there to aid activity. When using them alongside some stretching and strengthening exercises we are helping our children thrive in movement.
If you do decide to use Kidzoles please take advantage of the 25% off 1st pairs CODE. You’ll be emailed it once you sign up to Kidzoles Club newsletter on the SHOP page.